Perspective on Managing Right Ventricular Failure in the Perioperative Environment
Shirin Saeed, MD, Peva Gbagornah, MD, Mark Robitaille, MD
Published April 18, 2025 | Clinics in Medical Education
Issue 6 | Volume 1 | April 2025
Right ventricular (RV) function is significant for cardiac pump function, as it provides preload to the left ventricle and systemic circulation while maintaining interventricular interdependence. Acute right ventricular dysfunction (RVD) can occur perioperatively, often in patients with chronic ischemic or non-ischemic cardiomyopathies, chronic lung disease, pulmonary hypertension, or valvular conditions. For instance, one-third of heart failure patients with preserved left ventricular ejection fraction (LVEF) also exhibit RVD and the incidence rises to 48% when LVEF is reduced. Acute perioperative RVD may arise from sudden increases in RV afterload due to factors like pulmonary embolism, hypoxia, hypercapnia, or acidemia, or from decreased RV contractility resulting from conditions such as RV infarction, myocarditis, or post-cardiotomy shock. An accurate assessment of RV function is essential for preoperative risk stratification, determining the appropriate care setting, and managing intraoperative and postoperative care. Despite substantial evidence linking perioperative RVD to adverse clinical outcomes, there is a lack of published guidelines or recommendations to aid clinicians in conducting comprehensive, evidence-based assessments of RVD risk during the perioperative period.
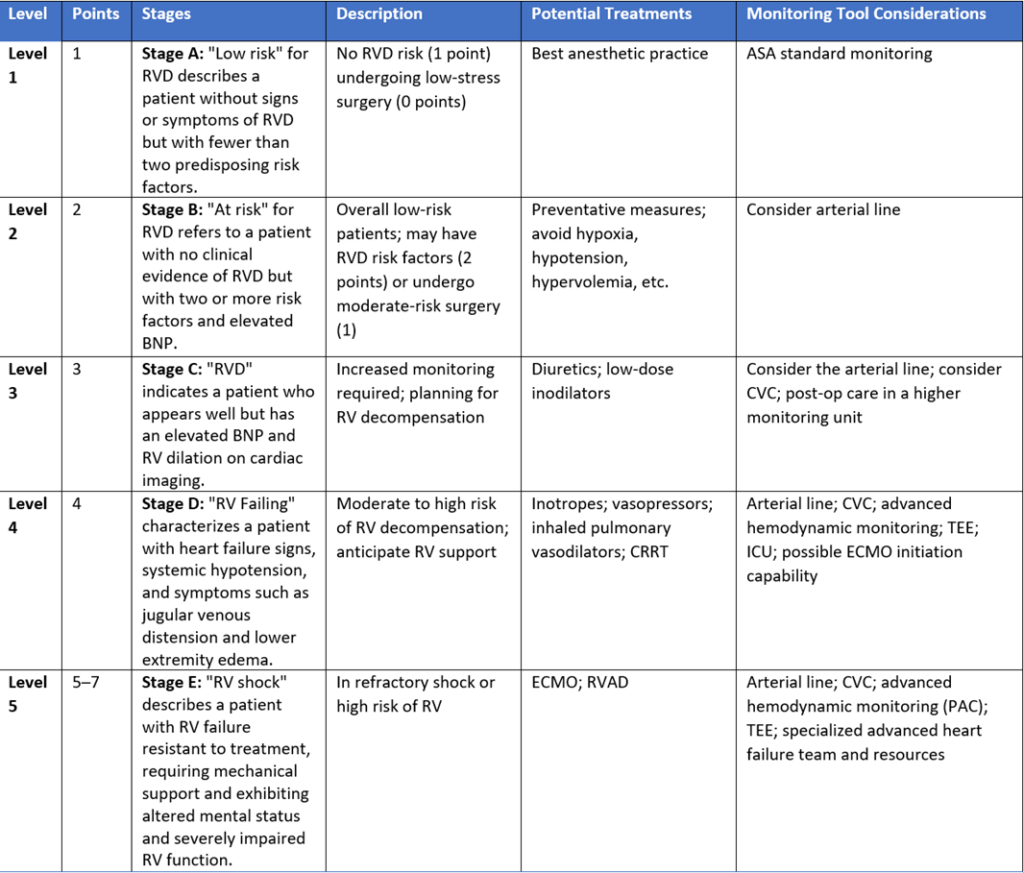
The POQI-IX group developed a consensus statement and stratified perioperative right ventricle function in five stages to screen and assess right ventricular function during the perioperative period. The “POQI 9 RV Risk Score” can be used to guide monitoring techniques and management.
Diagnostic Indicators on Echocardiography Assessment
The diagnosis of right ventricular (RV) dysfunction and failure in the perioperative setting involves identifying key indicators of RV failure.
Key Indicators Include:
- Signs of RV Dilation:
- D-shaping of the interventricular septum (IVS)
- Increased RV:LV diameter ratio
- Tricuspid regurgitation (TR)
- Signs of Impaired RV Systolic Function:
- Reduced Tricuspid Annular Plane Systolic Excursion (TAPSE)
- Signs of Elevated RV Preload:
- Plethoric inferior vena cava (IVC)
RV dilation is characterized by the bulging of the IVS into the LV, known as “D-shaping.” It is important to determine if this D-shaping occurs in diastole, systole, or both. Both systolic and diastolic D-shaping typically indicate RV pressure overload, while isolated diastolic D-shaping suggests RV volume overload. An increased RV:LV diameter ratio greater than 0.6 indicates RV dilation, with ratios above 1 indicating severe dilation. Severe dilation can lead to passive stretching of the tricuspid annulus, resulting in significant functional TR.TAPSE values below 17 mm are considered pathological and suggest impaired RV systolic function. However, in cases of severe TR, TAPSE may overestimate RV systolic function due to reduced afterload. After tricuspid valve annuloplasty, TAPSE may be significantly lower, leading to an underestimation of RV function; in such instances, RV fractional area change (FAC) may provide a more accurate assessment.

REFERENCES
1. O. Ibekwe, S., Deschamps, J., Grocott, M.P. et al. Perioperative Quality Initiative (POQI) consensus statement on perioperative assessment of right ventricular function. Perioper Med 12, 66 (2023).
2. Perioperative management of the vulnerable and failing right ventricle R. C. Arora1,7*, J. K. Brown2 , S. Chatterjee3,8, T. J. Gan4 , G. Singh5,9, M. Z. Tong6 and on behalf of the POQI IX Consortium