Regional Anesthesia and Acute Compartment Syndrome
Huma Syed Hussain, MD, Thy Vo, MD, Lisa Kunze, MD
Published April 18, 2025 | Clinics in Medical Education
Issue 6 | Volume 1 | April 2025
Case Summary:
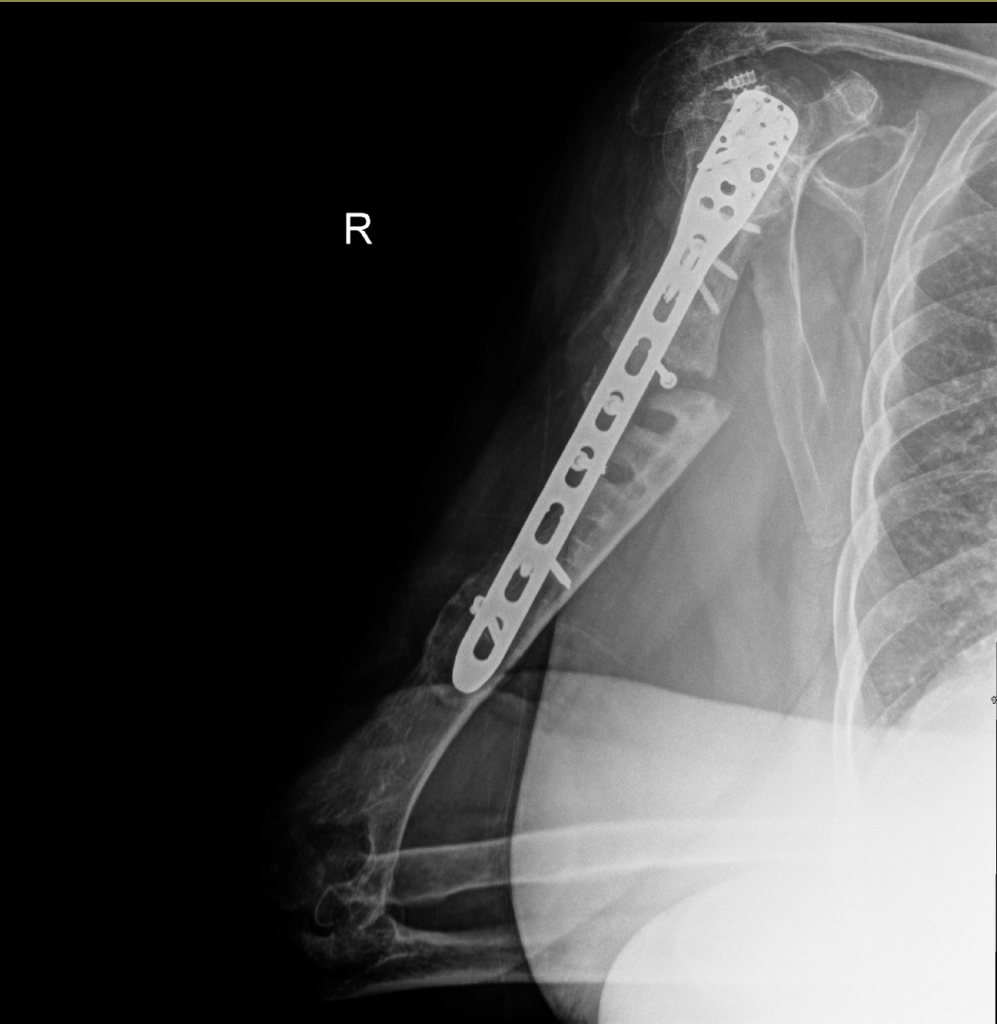
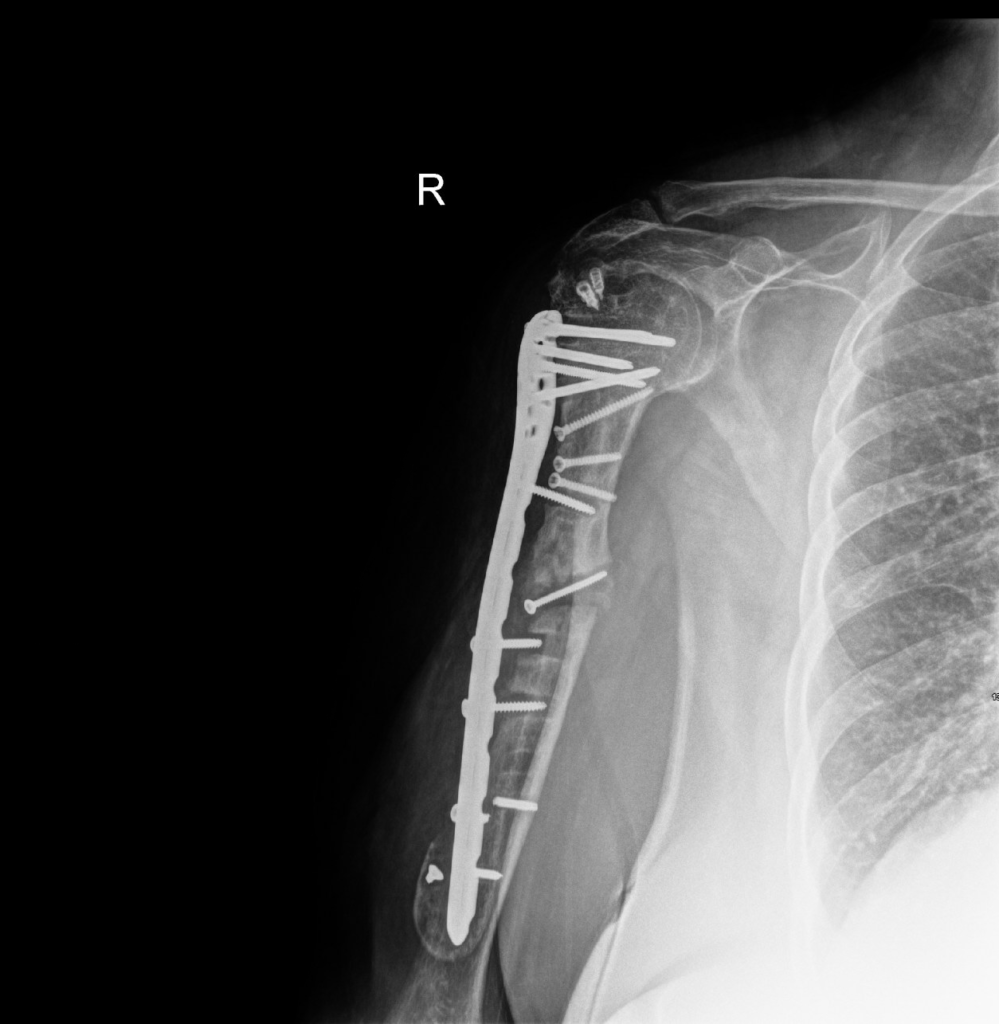
A 66-year-old individual with a complex medical and surgical history presented for right humerus open reduction and internal fixation (ORIF) due to a nonunion. The patient had undergone multiple prior attempts at ORIF, including an initial surgery performed at another facility, followed by a revision which was also unsuccessful.
Intubations for previous surgeries (hernia repair, humerus surgeries) had been uneventful, utilizing video laryngoscopy (McGrath) and a 7.0 endotracheal tube, with Grade 1 views achieved.
The patient had been evaluated preoperatively and cleared for surgery. The planned procedure was a repeat ORIF of a persistent nonunion of the right humerus.
A right supraclavicular peripheral nerve block was performed for postoperative pain management at the request of the surgical team. The procedure had been conducted under ultrasound guidance using a single-shot technique, and 17 mL of 0.5% bupivacaine had been administered. The injection had been completed without complications, with negative aspiration for blood, no paresthesia during injection, and appropriate visualization of local anesthetic spread around the nerve on ultrasound.
Acute Compartment Syndrome:
Acute compartment syndrome (ACS) is a surgical emergency in which rising pressure within a muscle compartment compromises tissue perfusion, potentially leading to irreversible muscle and nerve damage within hours. Prompt recognition and fasciotomy are essential to prevent long-term functional loss or limb-threatening complications. The diagnosis can be particularly challenging, as hallmark signs such as pain out of proportion to injury, tight compartments, and paresthesia are nonspecific and may be masked in certain settings.
The use of regional anesthesia (RA) for analgesia in trauma or orthopedic surgery has traditionally raised concern due to its potential to obscure the early signs of ACS, particularly in alert patients who would otherwise report disproportionate pain. However, this association remains controversial. Although case reports link prolonged nerve blocks with delayed ACS diagnosis, evidence also shows that ACS has been diagnosed and successfully managed in patients receiving single-shot or catheter-based RA.
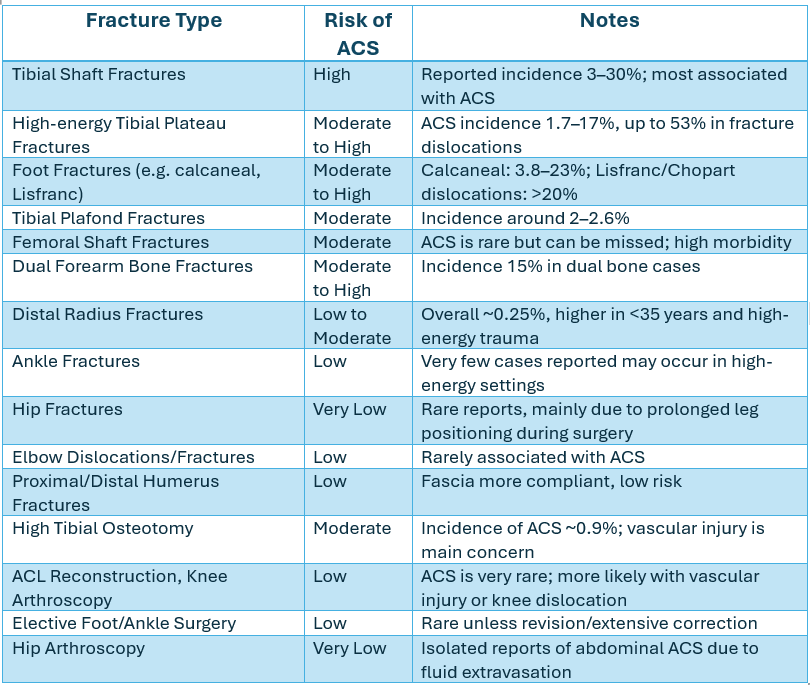
Upper limb fractures, including those of the humerus (proximal, shaft, and distal), are considered to have a low risk of ACS, largely due to the relatively compliant fascia and anatomical communication with the shoulder girdle, which accommodates swelling more easily than the lower limb.
Nevertheless, clinicians should remain vigilant postoperatively, especially in the setting of high-energy trauma, and ensure protocols are in place for timely reassessment should symptoms suggestive of ACS arise.
Clinical Consideration:
While regional anesthesia (RA) offers effective and opioid-sparing analgesia for orthopedic procedures, its use in settings where acute compartment syndrome (ACS) is a potential complication must be approached thoughtfully. Although RA is not absolutely contraindicated in these scenarios, certain high-risk fracture patterns, high-energy trauma, or complex surgical interventions may warrant caution. In such cases, RA should only be administered after a thorough risk-benefit discussion with the surgical team.
In the context of elective upper limb surgeries such as arthroscopic or open procedures of the shoulder, elbow, and wrist, the overall risk of ACS is considered very low. The large and anatomically connected compartments of the upper arm, such as the deltoid and arm compartments, help accommodate postoperative swelling. ACS in this setting is exceedingly rare and typically reported only in isolated case studies, often in the context of unusual surgical complexity or hematoma formation.
Given the low incidence of ACS in elective upper limb procedures, RA is considered safe and appropriate for most patients. However, providers should remain mindful that surgical complexity, anticoagulant use, and individual patient factors can still influence the risk profile. As with any anesthesia plan, clinical vigilance and close postoperative monitoring remain essential.
Reference
1. Dwyer, Tim et al. “Regional anesthesia and acute compartment syndrome: principles for practice.” Regional Anesthesia and Pain Medicine vol. 46,12 (2021): 1091-1099. doi:10.1136/rapm-2021-102735